Last month the Health and Social Care Information Centre published its latest statistics on the deprivation of liberty safeguards (DoLS). There was something of a dip in the number of applications in the last quarter of 2012 and the first quarter of 2013 (coincidentally, the first two quarters after the ruling in Cheshire West), and a general flattening of the year-on-year rise in applications:

This data release also showed that the extraordinary variability in the number of applications and authorisations under the DoLS between different supervisory bodies has continued into their fourth year*:
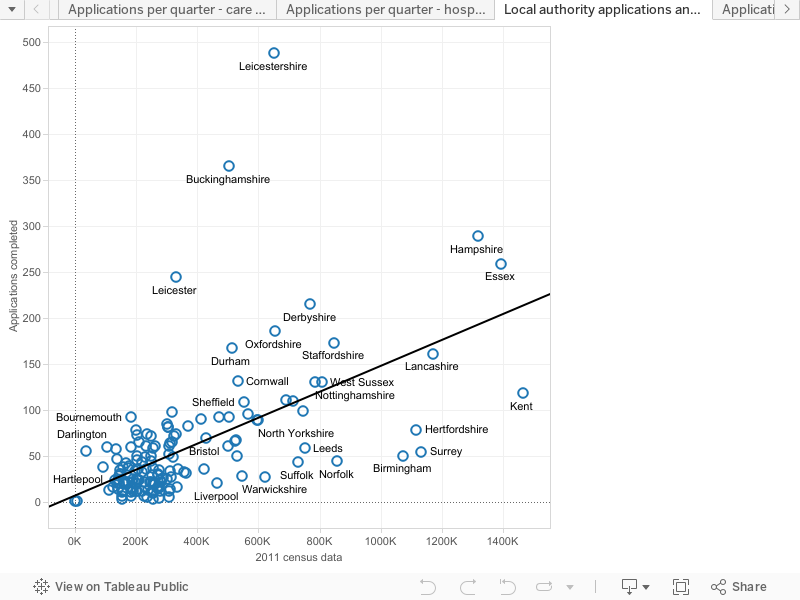

Replicating last year’s pattern of extreme variance, if you scaled up each local authority’s per-capita rate of DoLS applications in their area to reflect the size of England, the lowest per-capita authority (Kingston-Upon-Hull) would have received 620 applications, whereas Rutland would have received 78,024. That’s 125 times as many. (I will at some point be updating my statistical guide to the MCA to include these data, but I’m just waiting on a juicy FOI request for data on third party referrals and Part 8 reviews which I noticed the HSCIC has been collecting but not publishing...).
So – what is prompting this extreme variance? Could it be that people are 125 times more likely to be deprived of their liberty in Rutland than in Kingston-Upon-Hull? Or could it be, conversely, that people are 125 times more likely to be deprived of their liberty without safeguards in Kingston-Upon-Hull than Rutland? Or, could it be that the term ‘deprivation of liberty’ has frankly lost any semblance of an agreed upon meaning and so it has becoming a linguistic nonsense to say how many people are, or are not, deprived of their liberty in Rutland or Kingston-Upon-Hull, as nobody agrees upon what ‘deprivation of liberty’ even means?! As Charles J commented on BBC Radio 4's The Report, if you ask three people what it means, you will probably get four answers. What we can say, however, is that people in Rutland probably have better independent scrutiny of their care, and are more likely to be able access safeguards like advocacy and (in theory) the Court of Protection to protect their human rights, than the people of Kingston-Upon-Hull.
A major factor in the number of applications and authorisations under the DoLS in any given area is the definition of ‘deprivation of liberty’ that care home, local authority and hospital staff are labouring under there. In 2009, shortly after the DoLS were introduced, researchers asked best interests assessors, psychiatrists, IMCAs and lawyers with expertise in the DoLS to judge whether each of a set of 12 vignettes (derived from real-life clinical cases in hospital settings) constituted a deprivation of liberty. Famously, the study found agreement in only one case – and agreement across the other cases was ‘slight’ with a greater tendency to disagreement amongst the expert lawyers. Lawyers had the greatest tendency to think that a deprivation of liberty was occurring, followed by IMCAs, then best interests assessors and with psychiatrists being the least inclined to regard a person’s situation as a deprivation of liberty (Cairns, R., Brown, P., Grant-Peterkin, H., Owen, G. S., Richardson, G., Szmukler, G. & Hotopf, M. 'Mired in confusion: making sense of the Deprivation of Liberty Safeguards' (2011) Medicine, Science and the Law, 51(4) 228-236; Cairns, R., Brown, P., Grant-Peterkin, H., Khondoker, M. R., Owen, G. S., Richardson, G., Szmukler, G. & Hotopf, M. (2011) 'Judgements about deprivation of liberty made by various professionals: comparison study', The Psychiatrist, 35(9) 344-349). That study – fascinating though it was – is hard to generalise from: there have been many, many, more court cases defining what ‘deprivation of liberty’ means since the study was conducted, and the study focuses entirely on hospitals, whereas the majority of DoLS activity is in care homes. Moreover, the sample size is rather small (which is not a criticism - their method is hard to use with larger groups).
Recently, researchers at the University of Bristol conducted a similar – though not identical – study, exploring what factors influence the judgment of Best Interests Assessors (BIA’s) about whether a deprivation of liberty is, or is not, occurring (Carpenter, J., Langan, J., Patsios, D. & Jepson, M. (2013) 'Deprivation of Liberty Safeguards: What determines the judgements of Best Interests Assessors? A factorial survey', Journal of Social Work, Advance Access (DOI: 10.1177/1468017313504180)). The design of the study was different to the study by Cairns et al – instead of using vignettes based on case studies, and asking participants to specify what factors they felt influenced their judgments about deprivation of liberty (using a ‘nominal groups’ technique), the Bristol study generated artificial case studies by manipulating 10 pre-specified factors, which were chosen because they were thought to be relevant to decisions about deprivation of liberty. Vignettes were randomly generated based on these factors, which were then presented to a much larger participant group (93 BIA’s took part in the Bristol study; only 5 took part in Cairns’ et al’s). These participants selected whether they thought the cases described constituted a deprivation of liberty or not, were asked to rate their confidence on a scale of 1 (very confident) to 10 (Not at all confident) in that judgment. They were also asked whether there was any other information they would like to know before making a judgment, and whether case law had influenced their decision – and if so, how. The researchers were then able to quantify the impact of each factor on BIA's reasoning.
The findings of the Bristol study
The factors selected for experimental manipulation in the vignettes in the Bristol study do reflect key themes in case law, however – interestingly – their influence on the reasoning of BIA’s was not necessarily in line with what would be predicted by case law. I will take discuss each factor explored by the researchers in turn, and discuss the relevant case law.
Gender, Age (35, 48, 56, 70) and Condition (dementia; learning disabilities; alcohol-related brain damage; anxiety and delusional beliefs; acquired brain injury and physical disabilities) are, arguably, relevant to the ‘comparator’ approach adopted in Cheshire West. In fact, the researchers found no effect of gender, age or condition on the judgments of BIA’s. However one of the key problems with the ruling in Cheshire West is the level of specificity that is required in selecting the comparator; arguably these categories are too general to pick up a ‘comparator’ effect on reasoning.
Residence (registered care home; general hospital ward; hospital - mental health unit) is a key issue in the Court of Appeal ruling in P & Q, where Wilson LJ describes a ‘spectrum’ of normality in living arrangements, with living with one’s parents apparently being the most normal, through supported living, care homes and then large institutions like Bournewood hospital. Presumably living in a care home is more ‘normal’ than living in a general hospital ward or mental health unit, so one would expect to see an effect of residence on reasoning if BIA’s are applying the ruling in P & Q. However, the researchers found no effect of residence on judgments of BIA’s about whether a deprivation of liberty was occurring – I find this surprising, and it suggests that BIA’s may not be as influenced by P & Q on this issue as might be expected.
Objections and escape attempts (giving no verbal or physical indication of wishing to leave; saying ‘I feel like a prisoner here’ but making no attempt to leave’; frequently making purposeful attempts to walk out the door saying ‘I want to leave) are also a key factor in the ruling in P & Q, where Wilson LJ held that ‘the existence of objections is relevant to the objective element’. This line of case law has, however, not been very consistent. Notably, of course, HL in the original Bournewood case neither verbally objected nor attempted to leave, yet he was held to be deprived of his liberty. Meanwhile, subsequent to the ruling in P & Q, Jackson J found in C v Blackburn that a man who was both objecting and attempting to leave his care home by breaking the door down was not deprived of his liberty because he had nowhere else to go. Frustratingly, the existence or otherwise of somewhere else to go – which is also a key issue in Cheshire (see paragraph 58) is not a factor in this study.** And Baker J, in CC v KK, found that Mrs KK was not deprived of her liberty despite both objecting and having somewhere else to go, in part because ‘there is now little evidence that her overruled objections lead to a significant degree of conflict’ (and also the ‘relative normality’ of life in her care home). In short, the case law on objections is utterly contradictory. However, the BIA’s clearly treated this as a key factor (the second largest): ‘if the user frequently makes purposeful attempts to walk out, saying ‘I want to leave’, respondents were five times as likely to consider this evidence of a DoL, compared to giving no such indication’. This suggests that (overall) BIA’s are sticking to Wilson LJ’s template in P & Q and – by and large – ignoring the ruling in C v Blackburn. However, the likelihood of finding a deprivation of liberty was reduced if a person made no physical escape attempt and only expressed that ‘I feel like a prisoner here’ (this only increased judgments of deprivation of liberty twofold, rather than fivefold). This suggests that the ruling in CC v KK may be having some impact. It also suggests that people who are physically unable to attempt to leave are much less likely to benefit from the deprivation of liberty safeguards...
Distress (shows no distress; appears distressed but there is no known trigger; is distressed and agitated on a regular basis) was also discussed in P & Q, where in the High Court (then known as MIG & MEG) Parker J found that the happiness of the two young women was an indicator that they were not deprived of their liberty. In the Court of Appeal, Wilson LJ described happiness as ‘not relevant to whether she is deprived of her liberty’, but found that objections (discussed above) were. Of course, where a person’s verbal communication is impaired (or staff lack the skills to communicate with them, or the person is simply too cowed or institutionalised to formulate a recognisable objection), arguably distress should be interpreted as a possible objection – but the court did not consider this possibility in P & Q. Distress is not, then, necessarily a factor pointing to deprivation of liberty – according to the case law – but it might be if it were interpreted as an objection of some kind. The researchers found that if a person was showing signs of distress they BIA’s were twice as likely to identify a deprivation of liberty than if they were not. It would be interesting to know whether this was correlated with objections and escape attempts – whether distress simply increased the likelihood of finding deprivation of liberty where a person was also objecting or attempting to escape, or whether distress even in the absence of escape attempts and objections might increase the likelihood of deprivation of liberty being found.
Staff attempts to prevent a person from leaving (Do not take any action to prevent the person from leaving; Attempt to distract or verbally dissuade the person from leaving; Gently lead the person by hand away from exit; use coercive strategies to restrain the person from leaving the setting) has not been held to be a key factor in any domestic case. In Bournewood, the European Court of Human Rights emphasised that a person can be deprived of their liberty even when they have made no attempt to leave (and hence there has been no staff attempt to prevent them from leaving). In JE v DE, although Mr DE had frequently expressed a desire to leave, he had not physically attempted to, yet he was found to be deprived of his liberty. In P & Q, both young women would have been prevented from leaving or brought back if they left, but they were not found to be deprived of their liberty. In C v Blackburn with Darwen, Mr C had broken the door down attempting to leave, had been prevented from leaving by the police, but was not deprived of his liberty. In the European Cases – including Storck v Germany, and the 2012 trinity of ECHR cases, being prevented from leaving was, of course, a key factor, but the European case law is distinctly at odds with domestic rulings. In this study, however, staff attempts to prevent a person from leaving was the single biggest factor influencing BIA’s judgments about deprivation of liberty: ‘Respondents are almost six times as likely to state that staff using coercive strategies was a DoL, compared to not taking any coercive action.'
Medication (Not prescribed any mood altering medication; On a PRN dose of medication at times to reduce agitation and anxiety; On regular and high level doses of medication, including use of PRN, to reduce agitation and anxiety) is discussed in the ruling in P & Q, where Wilson LJ stated that ‘the administration to a person of medication, at any rate of antipsychotic drugs and other tranquilisers, is always a pointer towards the existence of the objective element: for it suppresses her liberty to express herself as she would otherwise wish’. I’ve always found this ruling bizarre, as having held that the administration of tranquilising medication is a pointer towards deprivation of liberty, Wilson LJ declines to consider whether Q (MEG)'s being administered Risperidone – a potent antipsychotic which has sedating effects - is a pointer towards her being deprived of her liberty. Similarly, C's mood was ‘is controlled by antipsychotic medication’ in C v Blackburn, yet he was not found to be deprived of his liberty. The BIA’s appear to have been influenced by what Wilson LJ said (as opposed to what he did), as ‘Respondents were nearly three times as likely to identify a DoL if the user was on regular and high level doses of medication, including use of PRN, to reduce agitation and anxiety, and nearly three times as likely if they were just on a PRN dose for the same reason.’
Staff supervision (no special supervision; Are aware of the person’s whereabouts at least every 3 to 4 hours; Supervise the person one-to-one; Accompany the person when out of home/ward) has been a key factor in ECHR rulings such as the Bournewood Judgment and the 2012 trinity – usually expressed in terms of ‘continuous supervision and control’. However, since the ruling in MIG & MEG, it has not been a key factor in the domestic case law. Not only MIG & MEG, but also P in Cheshire, Mr C in C v Blackburn, have been subject to high levels of staff supervision but have not been regarded as deprived of their liberty. Perhaps as a result of these rulings, staff supervision was a very weak predictor of BIA’s finding that a person was deprived of their liberty in this research. In comparison with situations where no supervision was in place, BIA’s were only 85% more likely (ie. just under two-fold) to identify deprivation of liberty for persons accompanied by staff when they are out of the care home or ward, and only 69% more likely for people with one:one supervision. This suggests that BIA’s reasoning in relation to supervision and control is in line with domestic case law, but sharply at odds with the ECHR.
Contact with outside world (Frequently goes out; Infrequently goes out; Rarely goes out) is not a determinative factor in either ECHR or domestic case law, but can be relevant. At the ECHR level, the fact that a person has contact with the outside world does not negate what would otherwise be a deprivation of liberty – the critical factor in the 2012 cases was the extent to which that contact was under the control of others. Domestically, contact with the outside world may be relevant to the ‘normality’ of a person’s situation. In P & Q, Wilson LJ says that the ‘enquiry into normality’ must take into account factors such as whether a (young) person goes to a school, college, day centre or work, etc. The researchers found that people who people who went our rarely or infrequently were twice as likely to be found to be deprived of their liberty by BIA’s than those who went out frequently.
Family views on care provided (Family are entirely happy with the care and treatment provided; Family are unhappy with some aspects of the care and treatment provided; Family are unhappy with all aspects of the care and treatment provided) is a difficult factor to pin down in terms of case law. The domestic case law has – since Neary v Hillingdon – been pretty consistent in finding that where a person’s family are asking for them to be returned to their care, they are likely to be deprived of their liberty. In Cheshire, having essentially said that if a person is subject to restrictions which are 'necessary' and 'normal' for people with a comparable condition, Munby LJ then went on to say that ‘Matters are, of course, very different where a person has somewhere else to go and wants to live there but is prevented from doing so by a coercive exercise of public authority’, and then referred to JE v DE, Neary v LB Hillingdon and the Bournewood case – all examples of where people’s families were asking for them to be returned to the family home. Yet the factor 'family views on care' doesn’t quite capture this important dimension – a family could be unhappy with a person’s care, yet not want them home, or they could feel that the care quality is fine, yet still want them home. The case C v A Local Authority (the infamous ‘blue room’ case) is a rare example of a person being said to be deprived of their liberty where they were not objecting, the family were not asking for them to return home, but the family were unhappy with the quality of the care. But the key issue there wasn’t that the family were unhappy, it’s that the care really was of such atrocious quality it constituted inhuman and degrading treatment and the restrictions were excessive. Meanwhile, in Strasbourg, the 2012 trinity of cases have all concerned people whose families were not at all bothered about the quality of care, nor were they asking for people to be returned home (much the opposite!) yet they were still said to be deprived of their liberty. In short, the domestic case law is more or less silent on family views on care, but strong on family wanting a person home, and the ECHR says neither factor is relevant. In this study, if family were unhappy with the care quality, BIA’s were two and a half times more likely to find that a deprivation of liberty was occurring.
The BIA’s stated that case law was influencing their decision making in 37% of vignettes, and one of the most commonly cited cases was Neary v Hillingdon. This is somewhat surprising as – as I’ve just discussed – the critical factor in Neary v Hillingdon was that Steven Neary was being prevented from returning to the care of his family, which is not a factor in the study. However, some BIA’s apparently took from Neary the message that if family were unhappy with the care a deprivation of liberty was more likely to be occurring. Unsurprisingly, Cheshire West and P & Q were also cited – reducing the impact of supervision and coercion on BIA’s judgments - and as I’ve discussed, there are signs of P & Q influenced reasoning around objections and medication. Despite the trend of domestic case law away from this factor, freedom to leave is still having a marked impact on BIA’s judgments.
Discussion
The researchers describe the use of case law in this study as ‘encouraging’. It certainly is encouraging that BIA’s are able to cite case law, which suggests that their professional training is keeping many of them up to date with important developments. However, the conclusion drawn by the researchers is rather more optimistic than I would have come to for one important reason: the BIA’s were overall very confident in their judgments regarding whether a deprivation of liberty is occurring (on average they rated their judgments a ‘3’). The fact is, to put it bluntly, nobody should be confidently in their judgments of whether a deprivation of liberty is occurring because – as this brief overview of the case law shows – the case law is utterly contradictory. The researchers found no effect of professional experience on confidence judgments – and this may be because the more experience one has of DoLS rulings, the more one will become attuned to their complex and often contradictory nature (not to mention their diversion from the ECHR case law). This echoes the finding of Cairns et al that unanimity as to what constitutes a deprivation of liberty was least amongst the expert lawyers – those who should have the greatest exposure to, and knowledge of, the case law.
The problem is this: the law is supposed to be ‘formulated with sufficient precision to enable the citizen to regulate his conduct’ (Sunday Times v UK). This is a fundamental principle of the ideal of the ‘rule of law’ – that constitutional safeguard against the despotism of rulers and the petty tyranny of bureaucrats. In short, the conduct of agents of the state should be regulated by the law, not by their own whims and caprices. The problem with DoLS is that there is simply so much scope for interpretation, so much scope for picking and choosing from a menu of contradictory rulings about what constitutes a deprivation of liberty, that it is impossible to reduce the variability of BIA’s decisions. This is reflected in the DoLS statistics I showed at the start of this post, but – worryingly – the confidence of BIA’s in their own decisions about the existence of deprivation of liberty suggests they may not be aware of the extent to which it is their own judgment, not the law, which is influencing them.
*NB: As these are data in the public domain, I have been experimenting with Tableau Public to make graphs – they are more flexible and a lot less ugly than SPSS... The downside is they come out rather messy on this blog because of their size - the plus side is that if you're a data geek you can now download it from Tableau and have a look at the other charts I made with it.
**In fairness to the researchers, it is quite possible the factors were selected prior to the ruling in Cheshire, where alternative residence achieved a new prominence as a factor.

This data release also showed that the extraordinary variability in the number of applications and authorisations under the DoLS between different supervisory bodies has continued into their fourth year*:
Replicating last year’s pattern of extreme variance, if you scaled up each local authority’s per-capita rate of DoLS applications in their area to reflect the size of England, the lowest per-capita authority (Kingston-Upon-Hull) would have received 620 applications, whereas Rutland would have received 78,024. That’s 125 times as many. (I will at some point be updating my statistical guide to the MCA to include these data, but I’m just waiting on a juicy FOI request for data on third party referrals and Part 8 reviews which I noticed the HSCIC has been collecting but not publishing...).
So – what is prompting this extreme variance? Could it be that people are 125 times more likely to be deprived of their liberty in Rutland than in Kingston-Upon-Hull? Or could it be, conversely, that people are 125 times more likely to be deprived of their liberty without safeguards in Kingston-Upon-Hull than Rutland? Or, could it be that the term ‘deprivation of liberty’ has frankly lost any semblance of an agreed upon meaning and so it has becoming a linguistic nonsense to say how many people are, or are not, deprived of their liberty in Rutland or Kingston-Upon-Hull, as nobody agrees upon what ‘deprivation of liberty’ even means?! As Charles J commented on BBC Radio 4's The Report, if you ask three people what it means, you will probably get four answers. What we can say, however, is that people in Rutland probably have better independent scrutiny of their care, and are more likely to be able access safeguards like advocacy and (in theory) the Court of Protection to protect their human rights, than the people of Kingston-Upon-Hull.
A major factor in the number of applications and authorisations under the DoLS in any given area is the definition of ‘deprivation of liberty’ that care home, local authority and hospital staff are labouring under there. In 2009, shortly after the DoLS were introduced, researchers asked best interests assessors, psychiatrists, IMCAs and lawyers with expertise in the DoLS to judge whether each of a set of 12 vignettes (derived from real-life clinical cases in hospital settings) constituted a deprivation of liberty. Famously, the study found agreement in only one case – and agreement across the other cases was ‘slight’ with a greater tendency to disagreement amongst the expert lawyers. Lawyers had the greatest tendency to think that a deprivation of liberty was occurring, followed by IMCAs, then best interests assessors and with psychiatrists being the least inclined to regard a person’s situation as a deprivation of liberty (Cairns, R., Brown, P., Grant-Peterkin, H., Owen, G. S., Richardson, G., Szmukler, G. & Hotopf, M. 'Mired in confusion: making sense of the Deprivation of Liberty Safeguards' (2011) Medicine, Science and the Law, 51(4) 228-236; Cairns, R., Brown, P., Grant-Peterkin, H., Khondoker, M. R., Owen, G. S., Richardson, G., Szmukler, G. & Hotopf, M. (2011) 'Judgements about deprivation of liberty made by various professionals: comparison study', The Psychiatrist, 35(9) 344-349). That study – fascinating though it was – is hard to generalise from: there have been many, many, more court cases defining what ‘deprivation of liberty’ means since the study was conducted, and the study focuses entirely on hospitals, whereas the majority of DoLS activity is in care homes. Moreover, the sample size is rather small (which is not a criticism - their method is hard to use with larger groups).
Recently, researchers at the University of Bristol conducted a similar – though not identical – study, exploring what factors influence the judgment of Best Interests Assessors (BIA’s) about whether a deprivation of liberty is, or is not, occurring (Carpenter, J., Langan, J., Patsios, D. & Jepson, M. (2013) 'Deprivation of Liberty Safeguards: What determines the judgements of Best Interests Assessors? A factorial survey', Journal of Social Work, Advance Access (DOI: 10.1177/1468017313504180)). The design of the study was different to the study by Cairns et al – instead of using vignettes based on case studies, and asking participants to specify what factors they felt influenced their judgments about deprivation of liberty (using a ‘nominal groups’ technique), the Bristol study generated artificial case studies by manipulating 10 pre-specified factors, which were chosen because they were thought to be relevant to decisions about deprivation of liberty. Vignettes were randomly generated based on these factors, which were then presented to a much larger participant group (93 BIA’s took part in the Bristol study; only 5 took part in Cairns’ et al’s). These participants selected whether they thought the cases described constituted a deprivation of liberty or not, were asked to rate their confidence on a scale of 1 (very confident) to 10 (Not at all confident) in that judgment. They were also asked whether there was any other information they would like to know before making a judgment, and whether case law had influenced their decision – and if so, how. The researchers were then able to quantify the impact of each factor on BIA's reasoning.
The findings of the Bristol study
The factors selected for experimental manipulation in the vignettes in the Bristol study do reflect key themes in case law, however – interestingly – their influence on the reasoning of BIA’s was not necessarily in line with what would be predicted by case law. I will take discuss each factor explored by the researchers in turn, and discuss the relevant case law.
Gender, Age (35, 48, 56, 70) and Condition (dementia; learning disabilities; alcohol-related brain damage; anxiety and delusional beliefs; acquired brain injury and physical disabilities) are, arguably, relevant to the ‘comparator’ approach adopted in Cheshire West. In fact, the researchers found no effect of gender, age or condition on the judgments of BIA’s. However one of the key problems with the ruling in Cheshire West is the level of specificity that is required in selecting the comparator; arguably these categories are too general to pick up a ‘comparator’ effect on reasoning.
Residence (registered care home; general hospital ward; hospital - mental health unit) is a key issue in the Court of Appeal ruling in P & Q, where Wilson LJ describes a ‘spectrum’ of normality in living arrangements, with living with one’s parents apparently being the most normal, through supported living, care homes and then large institutions like Bournewood hospital. Presumably living in a care home is more ‘normal’ than living in a general hospital ward or mental health unit, so one would expect to see an effect of residence on reasoning if BIA’s are applying the ruling in P & Q. However, the researchers found no effect of residence on judgments of BIA’s about whether a deprivation of liberty was occurring – I find this surprising, and it suggests that BIA’s may not be as influenced by P & Q on this issue as might be expected.
Objections and escape attempts (giving no verbal or physical indication of wishing to leave; saying ‘I feel like a prisoner here’ but making no attempt to leave’; frequently making purposeful attempts to walk out the door saying ‘I want to leave) are also a key factor in the ruling in P & Q, where Wilson LJ held that ‘the existence of objections is relevant to the objective element’. This line of case law has, however, not been very consistent. Notably, of course, HL in the original Bournewood case neither verbally objected nor attempted to leave, yet he was held to be deprived of his liberty. Meanwhile, subsequent to the ruling in P & Q, Jackson J found in C v Blackburn that a man who was both objecting and attempting to leave his care home by breaking the door down was not deprived of his liberty because he had nowhere else to go. Frustratingly, the existence or otherwise of somewhere else to go – which is also a key issue in Cheshire (see paragraph 58) is not a factor in this study.** And Baker J, in CC v KK, found that Mrs KK was not deprived of her liberty despite both objecting and having somewhere else to go, in part because ‘there is now little evidence that her overruled objections lead to a significant degree of conflict’ (and also the ‘relative normality’ of life in her care home). In short, the case law on objections is utterly contradictory. However, the BIA’s clearly treated this as a key factor (the second largest): ‘if the user frequently makes purposeful attempts to walk out, saying ‘I want to leave’, respondents were five times as likely to consider this evidence of a DoL, compared to giving no such indication’. This suggests that (overall) BIA’s are sticking to Wilson LJ’s template in P & Q and – by and large – ignoring the ruling in C v Blackburn. However, the likelihood of finding a deprivation of liberty was reduced if a person made no physical escape attempt and only expressed that ‘I feel like a prisoner here’ (this only increased judgments of deprivation of liberty twofold, rather than fivefold). This suggests that the ruling in CC v KK may be having some impact. It also suggests that people who are physically unable to attempt to leave are much less likely to benefit from the deprivation of liberty safeguards...
Distress (shows no distress; appears distressed but there is no known trigger; is distressed and agitated on a regular basis) was also discussed in P & Q, where in the High Court (then known as MIG & MEG) Parker J found that the happiness of the two young women was an indicator that they were not deprived of their liberty. In the Court of Appeal, Wilson LJ described happiness as ‘not relevant to whether she is deprived of her liberty’, but found that objections (discussed above) were. Of course, where a person’s verbal communication is impaired (or staff lack the skills to communicate with them, or the person is simply too cowed or institutionalised to formulate a recognisable objection), arguably distress should be interpreted as a possible objection – but the court did not consider this possibility in P & Q. Distress is not, then, necessarily a factor pointing to deprivation of liberty – according to the case law – but it might be if it were interpreted as an objection of some kind. The researchers found that if a person was showing signs of distress they BIA’s were twice as likely to identify a deprivation of liberty than if they were not. It would be interesting to know whether this was correlated with objections and escape attempts – whether distress simply increased the likelihood of finding deprivation of liberty where a person was also objecting or attempting to escape, or whether distress even in the absence of escape attempts and objections might increase the likelihood of deprivation of liberty being found.
Staff attempts to prevent a person from leaving (Do not take any action to prevent the person from leaving; Attempt to distract or verbally dissuade the person from leaving; Gently lead the person by hand away from exit; use coercive strategies to restrain the person from leaving the setting) has not been held to be a key factor in any domestic case. In Bournewood, the European Court of Human Rights emphasised that a person can be deprived of their liberty even when they have made no attempt to leave (and hence there has been no staff attempt to prevent them from leaving). In JE v DE, although Mr DE had frequently expressed a desire to leave, he had not physically attempted to, yet he was found to be deprived of his liberty. In P & Q, both young women would have been prevented from leaving or brought back if they left, but they were not found to be deprived of their liberty. In C v Blackburn with Darwen, Mr C had broken the door down attempting to leave, had been prevented from leaving by the police, but was not deprived of his liberty. In the European Cases – including Storck v Germany, and the 2012 trinity of ECHR cases, being prevented from leaving was, of course, a key factor, but the European case law is distinctly at odds with domestic rulings. In this study, however, staff attempts to prevent a person from leaving was the single biggest factor influencing BIA’s judgments about deprivation of liberty: ‘Respondents are almost six times as likely to state that staff using coercive strategies was a DoL, compared to not taking any coercive action.'
Medication (Not prescribed any mood altering medication; On a PRN dose of medication at times to reduce agitation and anxiety; On regular and high level doses of medication, including use of PRN, to reduce agitation and anxiety) is discussed in the ruling in P & Q, where Wilson LJ stated that ‘the administration to a person of medication, at any rate of antipsychotic drugs and other tranquilisers, is always a pointer towards the existence of the objective element: for it suppresses her liberty to express herself as she would otherwise wish’. I’ve always found this ruling bizarre, as having held that the administration of tranquilising medication is a pointer towards deprivation of liberty, Wilson LJ declines to consider whether Q (MEG)'s being administered Risperidone – a potent antipsychotic which has sedating effects - is a pointer towards her being deprived of her liberty. Similarly, C's mood was ‘is controlled by antipsychotic medication’ in C v Blackburn, yet he was not found to be deprived of his liberty. The BIA’s appear to have been influenced by what Wilson LJ said (as opposed to what he did), as ‘Respondents were nearly three times as likely to identify a DoL if the user was on regular and high level doses of medication, including use of PRN, to reduce agitation and anxiety, and nearly three times as likely if they were just on a PRN dose for the same reason.’
Staff supervision (no special supervision; Are aware of the person’s whereabouts at least every 3 to 4 hours; Supervise the person one-to-one; Accompany the person when out of home/ward) has been a key factor in ECHR rulings such as the Bournewood Judgment and the 2012 trinity – usually expressed in terms of ‘continuous supervision and control’. However, since the ruling in MIG & MEG, it has not been a key factor in the domestic case law. Not only MIG & MEG, but also P in Cheshire, Mr C in C v Blackburn, have been subject to high levels of staff supervision but have not been regarded as deprived of their liberty. Perhaps as a result of these rulings, staff supervision was a very weak predictor of BIA’s finding that a person was deprived of their liberty in this research. In comparison with situations where no supervision was in place, BIA’s were only 85% more likely (ie. just under two-fold) to identify deprivation of liberty for persons accompanied by staff when they are out of the care home or ward, and only 69% more likely for people with one:one supervision. This suggests that BIA’s reasoning in relation to supervision and control is in line with domestic case law, but sharply at odds with the ECHR.
Contact with outside world (Frequently goes out; Infrequently goes out; Rarely goes out) is not a determinative factor in either ECHR or domestic case law, but can be relevant. At the ECHR level, the fact that a person has contact with the outside world does not negate what would otherwise be a deprivation of liberty – the critical factor in the 2012 cases was the extent to which that contact was under the control of others. Domestically, contact with the outside world may be relevant to the ‘normality’ of a person’s situation. In P & Q, Wilson LJ says that the ‘enquiry into normality’ must take into account factors such as whether a (young) person goes to a school, college, day centre or work, etc. The researchers found that people who people who went our rarely or infrequently were twice as likely to be found to be deprived of their liberty by BIA’s than those who went out frequently.
Family views on care provided (Family are entirely happy with the care and treatment provided; Family are unhappy with some aspects of the care and treatment provided; Family are unhappy with all aspects of the care and treatment provided) is a difficult factor to pin down in terms of case law. The domestic case law has – since Neary v Hillingdon – been pretty consistent in finding that where a person’s family are asking for them to be returned to their care, they are likely to be deprived of their liberty. In Cheshire, having essentially said that if a person is subject to restrictions which are 'necessary' and 'normal' for people with a comparable condition, Munby LJ then went on to say that ‘Matters are, of course, very different where a person has somewhere else to go and wants to live there but is prevented from doing so by a coercive exercise of public authority’, and then referred to JE v DE, Neary v LB Hillingdon and the Bournewood case – all examples of where people’s families were asking for them to be returned to the family home. Yet the factor 'family views on care' doesn’t quite capture this important dimension – a family could be unhappy with a person’s care, yet not want them home, or they could feel that the care quality is fine, yet still want them home. The case C v A Local Authority (the infamous ‘blue room’ case) is a rare example of a person being said to be deprived of their liberty where they were not objecting, the family were not asking for them to return home, but the family were unhappy with the quality of the care. But the key issue there wasn’t that the family were unhappy, it’s that the care really was of such atrocious quality it constituted inhuman and degrading treatment and the restrictions were excessive. Meanwhile, in Strasbourg, the 2012 trinity of cases have all concerned people whose families were not at all bothered about the quality of care, nor were they asking for people to be returned home (much the opposite!) yet they were still said to be deprived of their liberty. In short, the domestic case law is more or less silent on family views on care, but strong on family wanting a person home, and the ECHR says neither factor is relevant. In this study, if family were unhappy with the care quality, BIA’s were two and a half times more likely to find that a deprivation of liberty was occurring.
The BIA’s stated that case law was influencing their decision making in 37% of vignettes, and one of the most commonly cited cases was Neary v Hillingdon. This is somewhat surprising as – as I’ve just discussed – the critical factor in Neary v Hillingdon was that Steven Neary was being prevented from returning to the care of his family, which is not a factor in the study. However, some BIA’s apparently took from Neary the message that if family were unhappy with the care a deprivation of liberty was more likely to be occurring. Unsurprisingly, Cheshire West and P & Q were also cited – reducing the impact of supervision and coercion on BIA’s judgments - and as I’ve discussed, there are signs of P & Q influenced reasoning around objections and medication. Despite the trend of domestic case law away from this factor, freedom to leave is still having a marked impact on BIA’s judgments.
Discussion
The researchers describe the use of case law in this study as ‘encouraging’. It certainly is encouraging that BIA’s are able to cite case law, which suggests that their professional training is keeping many of them up to date with important developments. However, the conclusion drawn by the researchers is rather more optimistic than I would have come to for one important reason: the BIA’s were overall very confident in their judgments regarding whether a deprivation of liberty is occurring (on average they rated their judgments a ‘3’). The fact is, to put it bluntly, nobody should be confidently in their judgments of whether a deprivation of liberty is occurring because – as this brief overview of the case law shows – the case law is utterly contradictory. The researchers found no effect of professional experience on confidence judgments – and this may be because the more experience one has of DoLS rulings, the more one will become attuned to their complex and often contradictory nature (not to mention their diversion from the ECHR case law). This echoes the finding of Cairns et al that unanimity as to what constitutes a deprivation of liberty was least amongst the expert lawyers – those who should have the greatest exposure to, and knowledge of, the case law.
The problem is this: the law is supposed to be ‘formulated with sufficient precision to enable the citizen to regulate his conduct’ (Sunday Times v UK). This is a fundamental principle of the ideal of the ‘rule of law’ – that constitutional safeguard against the despotism of rulers and the petty tyranny of bureaucrats. In short, the conduct of agents of the state should be regulated by the law, not by their own whims and caprices. The problem with DoLS is that there is simply so much scope for interpretation, so much scope for picking and choosing from a menu of contradictory rulings about what constitutes a deprivation of liberty, that it is impossible to reduce the variability of BIA’s decisions. This is reflected in the DoLS statistics I showed at the start of this post, but – worryingly – the confidence of BIA’s in their own decisions about the existence of deprivation of liberty suggests they may not be aware of the extent to which it is their own judgment, not the law, which is influencing them.
*NB: As these are data in the public domain, I have been experimenting with Tableau Public to make graphs – they are more flexible and a lot less ugly than SPSS... The downside is they come out rather messy on this blog because of their size - the plus side is that if you're a data geek you can now download it from Tableau and have a look at the other charts I made with it.
**In fairness to the researchers, it is quite possible the factors were selected prior to the ruling in Cheshire, where alternative residence achieved a new prominence as a factor.
No comments:
Post a Comment